
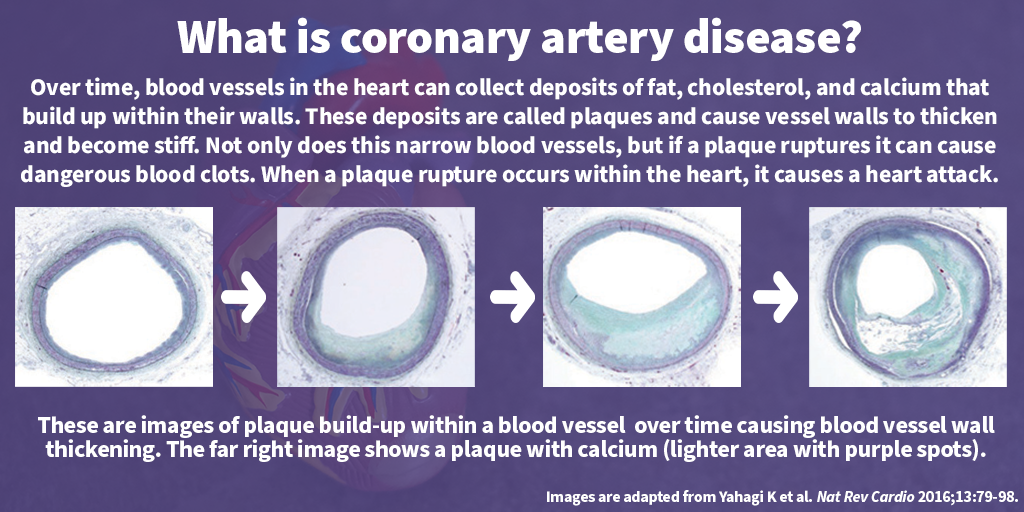
Chest pain is one of the most common symptoms that cause people to visit the emergency department. Because chest pain is a prevalent, non-specific symptom, doctors may have to perform numerous tests to determine the underlying cause. But what if there was a test that could rule out one of the reasons — coronary artery disease — for the next seven years?
CHÉOS’ Program Head for Emergency Medicine Dr. Frank Scheuermeyer, alongside St. Paul’s Hospital Radiologist and Canada Research Chair Dr. Jonathan Leipsic, published work showing that imaging the heart using coronary computed tomographic angiography (CCTA) is a valuable new tool in determining whether or not patients will have serious cardiac events in the future. Of the 459 chest pain patients in the emergency department who had CCTA showing no or minimal blockages in the arteries of their heart, none had a heart attack or died of cardiovascular disease over the next 7.5 years, and only two needed invasive heart procedures.

“The advantage of CCTA is that it is really definitive. If a patient comes in with mild chest pain and receives imaging that shows they don’t have significant coronary disease, there is a warranty that lasts over seven years,” said Dr. Leipsic, Professor of Radiology and Cardiology at UBC.
What is CCTA?
CCTA refers to specialized, high-resolution cardiac imaging that can visualize the blood vessels in the heart. St. Paul’s Hospital received the first public CCTA scanner in Canada which is especially useful as a diagnostic tool in patients with coronary artery disease. The combination of x-rays and computer technology used in CCTA can detect plaques, particularly softer ones that are typically more challenging to find.
The procedure itself is very quick, with the scanner taking about 12 seconds to collect the necessary images. Due to the precise nature of CCTA imaging, it is possible to determine the exact extent of blood vessel blockage in the heart.
Drs. Scheuermeyer and Leipsic’s research is very timely as the American College of Cardiology and the American Heart Association recently updated their chest pain guidelines citing CCTA as the gold standard method for imaging patients in both acute and stable settings.
Conventional stress testing has less warranty

Traditional stress testing involves a patient walking or running on a treadmill for up to 12 minutes, or injecting small amounts of radioactive dye. Both methods can provide signals that there is heart disease. Although stress testing is important when evaluating a patient’s exercise tolerance and looking for working heart muscle tissue when a patient has known coronary disease, it is not predictive.
“There’s less warranty with a stress test,” emphasized Dr. Scheuermeyer. “A patient can develop heart disease anytime between a couple of months or a couple of years after an apparently normal stress test. CCTA is useful for both patients and physicians because if a patient has chest pain and CCTA shows only mild coronary artery disease, it is extremely unlikely that the patient will progress to more serious heart disease. If patients have recurrent chest pain, physicians don’t have to start their investigation from scratch. Not only can this reduce patient anxiety, concern, and apprehension, but it also reduces resource use.”

Compared with stress testing, which requires further investigation if the results are abnormal, CCTA takes little time with images of the heart vessels captured over just a couple heartbeats. Furthermore, although CCTA and stress testing both expose patients to low levels of radiation, it is not unusual for patients to need numerous stress tests if they regularly experience chest pain.
“CCTA provides a definitive test result that is conclusive for years, which stress tests are not able to provide,” said Dr. Scheuermeyer, who is a Clinical Associate Professor in the Department of Emergency Medicine at UBC. Also, lying down for imaging as opposed to actively exercising for a diagnostic test is both more appealing and more accessible to patients.
Future directions
Although CCTA is a very helpful tool, it is not widely available. Future research could involve using CCTA in conjunction with a more available prognostic tool, biomarkers.
Biomarkers are detectable molecules found in the body that signal disease or damage. In heart disease, cardiac troponins — important protein components of heart muscle tissue — are commonly used biomarkers to indicate heart damage. Dr. Leipsic is currently working to determine whether or not certain levels of specific cardiac troponins could correlate with CCTA outcomes. This opens the possibility to associate low levels of cardiac biomarkers with what is being seen on CCTA, adding precision to prognostic estimates.
Overall, CCTA has many advantages over conventional stress testing when used for patients admitted to the emergency department with chest pain. Dr. Leipsic affirmed, “The long-term warranty provided by CCTA is unique. If a patient doesn’t have coronary disease, their outcomes are excellent.”
Co-authors of this study include CHÉOS Scientists Drs. Eric Grafstein, Jim Christenson, and Brian Grunau.


